
What is endometriosis?
"I’m not here to give you a medical lecture. What matters to me is making endometriosis understandable, in a way that is accessible, clear, and human. Because knowledge is power.
For individuals living with endometriosis, understanding the condition is a crucial step toward empowerment, toward navigating care, making informed decisions, and living better with the disease.
For organizations, healthcare professionals, and policymakers, understanding endometriosis clearly is essential to designing better patient pathways, stronger awareness campaigns, and more effective policies.
Empowerment begins with clarity.
And clarity begins with understanding"
- Laura Lequeu
Endometriosis is a multi-systemic (because it can affect different systems: urinary, digestive, pulmonary, neurvous, etc.), chronic and inflammatory disease that affects 1 to 2 women* out of 10. Worldwide, the average diagnostic delay ranges from 7 to 12 years.
According to the most widely accepted scientific theory, endometriosis can begin as early as the first menstruation, through what is known as retrograde menstruation (Sampson’s theory). However, alternative research suggests that in some cases the disease may originate much earlier in life, potentially during embryonic development, based on the Müllerian embryonic remnant theory.
I share these different hypotheses to highlight the complexity of endometriosis and the fact that science is still working to fully understand its origins. Research in this field is advancing, but it remains incomplete. We will need further studies (and patience) before having clearer and more definitive answers. However, endometriosis is increasingly regarded as a multifactorial disease, involving genetic, hormonal, immune, inflammatory, and potentially bacterial and environmental factors, a complexity we will explore further below.
Because this disease is hormone-dependent, without proper management from the very first symptoms, it can be progressive and cause significant pain and/or short- and/or long-term complications.
Although we mainly refer to endometriosis here, this also includes adenomyosis, often described as the “little cousin” of endometriosis. While closely related, it has some specific characteristics, as well as slightly different symptoms and diagnostic approaches. We can talk about it together.
*Laura intentionally alternates between the terms “women” and “individuals.” While endometriosis predominantly affects cisgender women, Laura is aware that the condition can also affect people who identify as FINTA, an acronym referring to women, intersex, non-binary, trans, and agender individuals. For Laura, inclusive language is important. It allows her to acknowledge both the biological reality of the disease and the diversity of people who may be affected by it.
To properly understand endometriosis, we must first understand how a human body with a uterus functions.
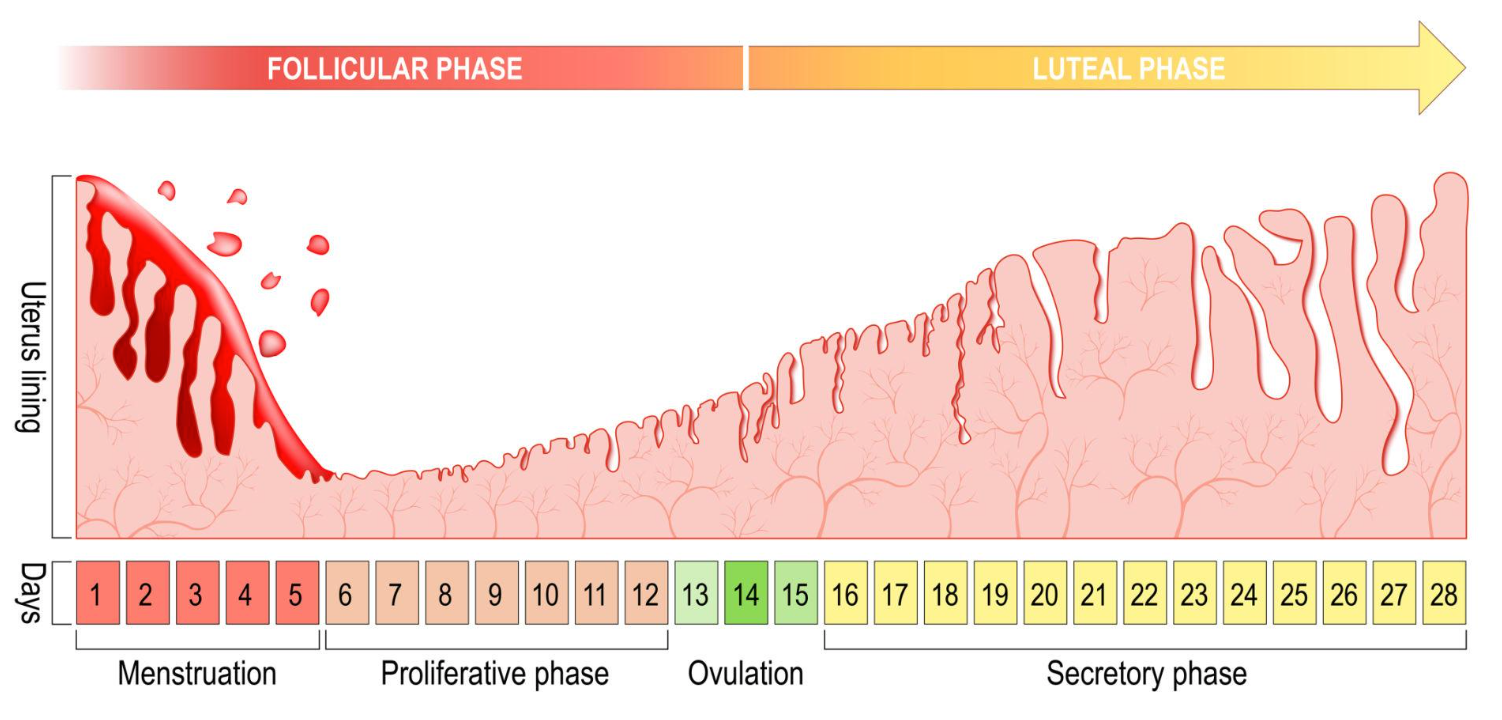
Throughout the menstrual cycle (a menstrual cycle begins on the first day of the period and ends on the first day of the next period; it lasts on average 28 days, although this can vary from one body to another), the endometrium (the tissue that lines the inner wall of the uterus, you can think of it a bit like wallpaper covering the inside of your uterus) gradually thickens throughout the cycle in order to welcome a potential embryo (in other words, a possible pregnancy).
If, at the end of the cycle, fertilization has not occurred, then the endometrium (which is the “nest” where the embryo would normally implant) is no longer needed and naturally breaks down through bleeding. This is what we more commonly call a period.
In principle, this process repeats itself every month until menopause.
In individuals with endometriosis, cells similar to the endometrium migrate…
By being drawn up through the Fallopian tubes, these cells then escape through the space between the end of the Fallopian tubes and the ovaries, as this space is not completely sealed, and they subsequently implant outside of their usual place, which is supposed to be the uterus (these cells can therefore implant on the reproductive system, the urinary system, the digestive system, the pulmonary system, etc.), and this is what we refer to as endometriosis.
However, there is another form of endometriosis called adenomyosis. In this specific case, these cells can infiltrate the myometrium (which is the uterine muscle, therefore inside the uterus), and this is referred to as adenomyosis, in other words, the cousin of endometriosis.
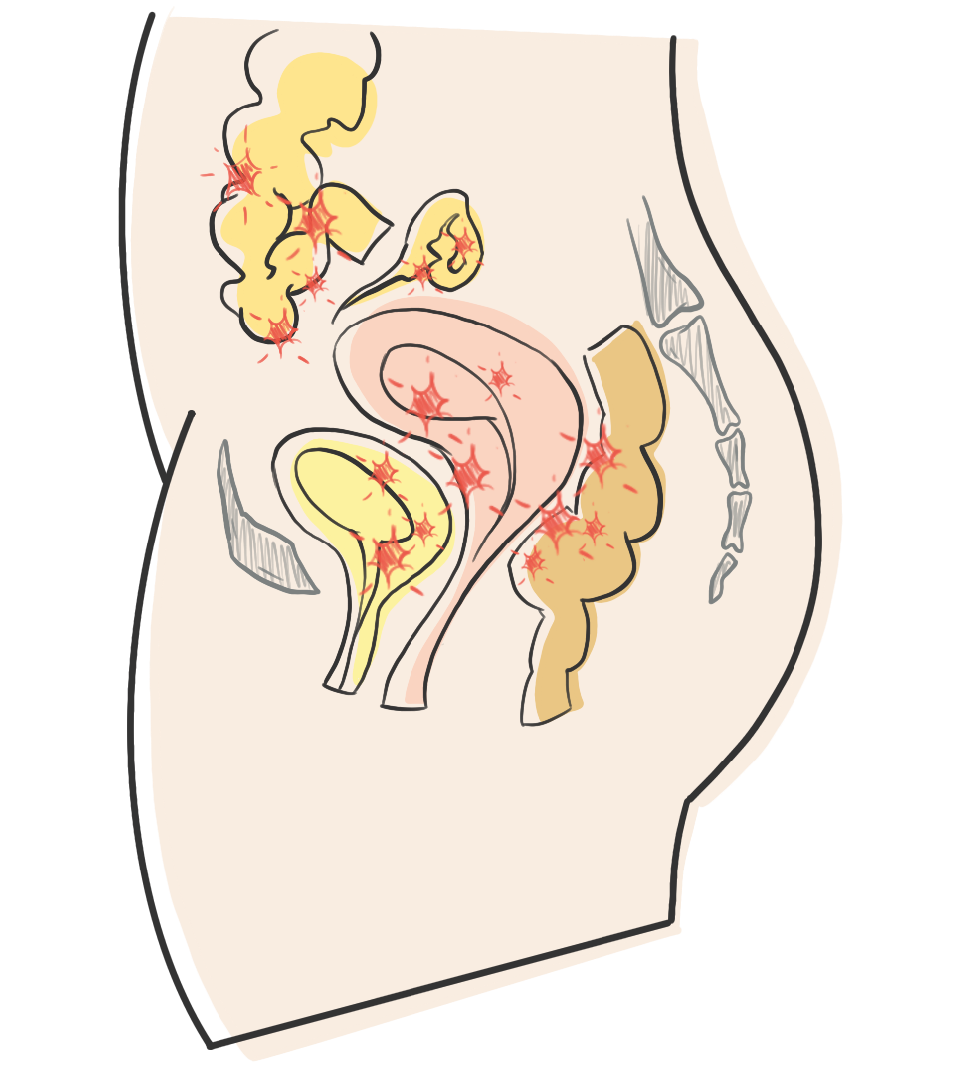
These endometrium-like cells become lesions, implants, or nodules of endometriosis and are most often located in the lower abdomen: on the peritoneum (which is a membrane covering the abdominal organs), on the ovaries, on or within the intestine or the bladder, more rarely on other organs (diaphragm, pleura, lungs), but also on the nervous system (non-exhaustive list).
There is no organ where endometriosis has not been found… It’s incredible, isn’t it?
This theory is the most widely accepted scientifically, but it has become increasingly controversial over the years as new discoveries emerge.
Indeed, the theory of retrograde menstruation was first introduced by John A. Sampson as early as 1921. This theory helps explain the asymmetrical and seemingly random distribution of lesions, which predominantly occur in the posterior compartment of the pelvis and mostly on the left side.
However, this theory clearly does not explain many forms of endometriosis, particularly those located in extra-pelvic sites.
Further research are therefore necessary, and we will need to remain patient as science continues to investigate and refine our understanding of the disease.
Note: All factors that promote retrograde menstruation (early menarche, short menstrual cycles, heavy menstrual bleeding, menorrhagia, etc.) increase the risk of endometriosis.
Therefore, other hypotheses and research avenues exist that may help explain endometriosis.
Genetic / hereditary factors
There is a fivefold higher risk of developing endometriosis among first-degree relatives (for example, from a mother to her daughter) compared to the general population. In addition, certain genetic variants play either a facilitating or an inhibitory role in the development of endometriosis.
Metaplastic factors
Endometriosis may occur when a generic tissue transforms into a specialized tissue in a location different from where it is normally supposed to be. Theories include:
- Coelomic metaplasia
- Hormonal or immunological factors
- Remnants of the Müllerian ducts
- Stem cell differentiation
Metastatic theory (transplantation / induction theory)
During menstruation, various blood or lymphatic vessels may draw endometrial cells into the circulation, allowing them to spread throughout the body.
Autoimmune hypothesis
Numerous abnormalities of the immune system have been identified in individuals with endometriosis, although no endometriosis-specific antibodies have ever been clearly demonstrated.
Infectious hypothesis
A recent discovery suggests a potential pathogenic role of bacteria from the genus Fusobacterium in the development of ovarian endometriosis (with possible antibiotic treatment). In addition, correlations have been observed between imbalances in the vaginal microbiome and the onset of endometriosis.
Environmental hypothesis:nvironnementale
One hypothesis considers the role of exposure to certain toxic substances or pollutants (particularly endocrine disruptors), potentially even in utero (that is, while we are still developing inside the uterus before birth).
All of this may seem complex. We said we would keep things simple here and that remains the goal.
But unfortunately, it is difficult to simplify what science itself has not yet fully clarified.
For deeper discussions or tailored explanations,
Laura can address your questions during a session or event.
Regarding the types of endometriosis, there are three main forms:
Note: It is important to understand that there is no correlation between the type or stage of endometriosis and the intensity of pain.
One can have a “very small” superficial stage 1 endometriosis and experience an extremely disabling quality of life due to the pain and/or symptoms it may cause.
Likewise, one can have a “severe” deep stage 4 endometriosis and experience no pain at all.
However, in order to better understand the extent of the disease (but again, not the level of pain!), two classifications exist: the type and the stage of endometriosis.
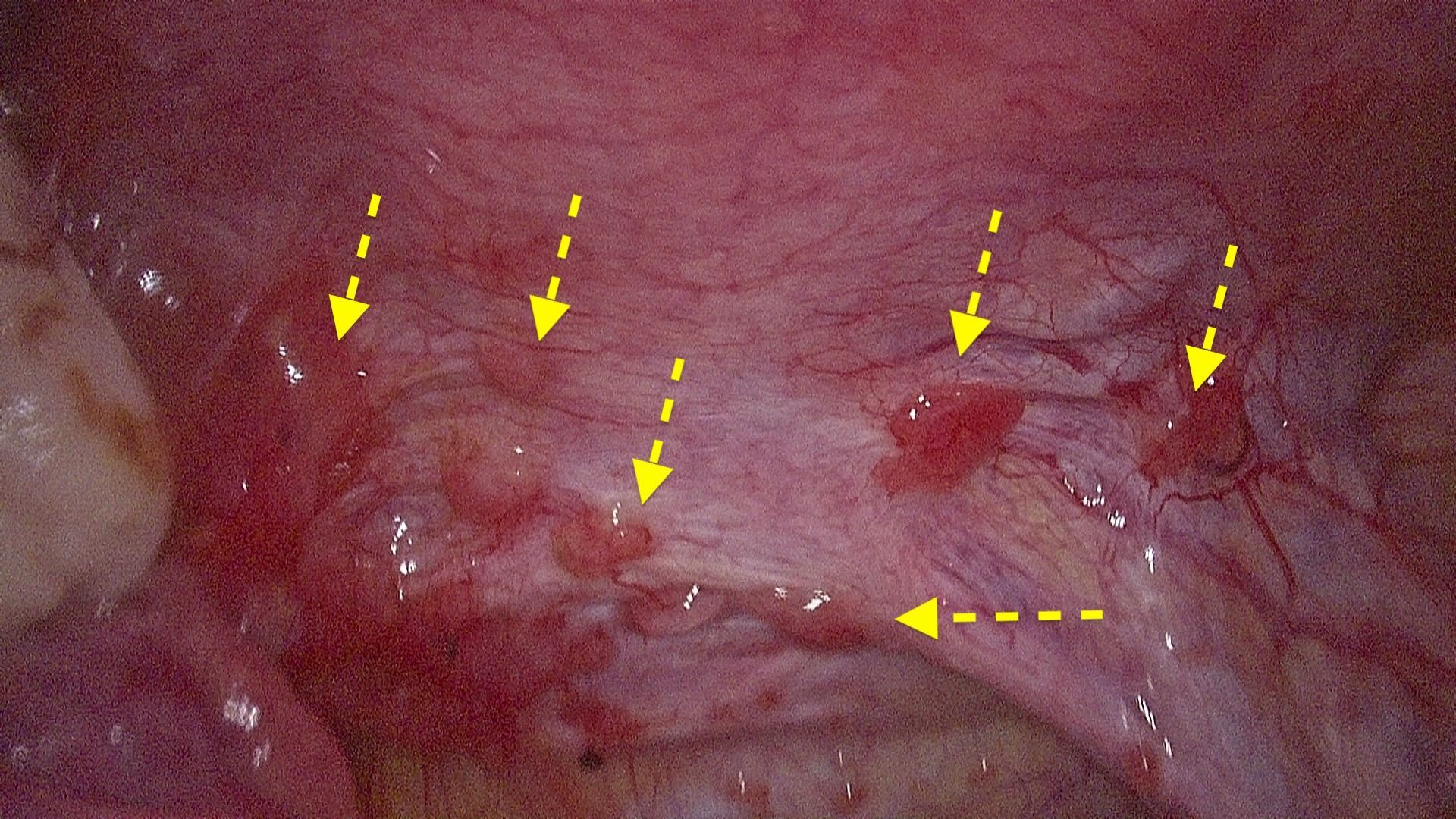
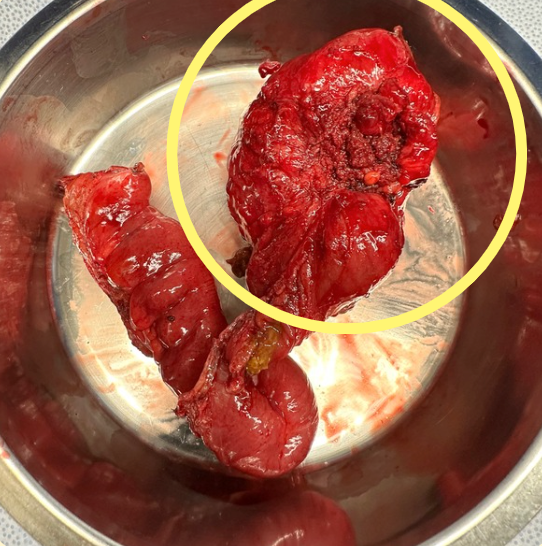
TW: By hovering over the magnifying glass icon, surgical images will appear.
01
Superficial (peritoneal) endometriosis:
on parle d’endométriose superficielle lorsque les lésions restent en superficie, à la surface du péritoine (membrane qui recouvre les organes de la cavité abdominale) . Elles peuvent prendre la forme de kystes (de quelques millimètres à quelques centimètres) en surface des tissus.

02
Ovarian cysts (endometriomas)
Endometriosis is considered ovarian when one or more endometriotic cysts develop on the ovary. These are referred to as endometriomas, also known as “chocolate cysts,” because they are cysts filled with old, coagulated blood whose color gradually turns dark brown, similar to chocolate.
This type of endometriosis directly affects the ovarian reserve and therefore has a more direct impact on the patient’s fertility.

03
Deep endometriosis (DIE)
Endometriosis is considered deep or infiltrating when lesions extend more than 5 millimeters beneath the surface (as opposed to superficial endometriosis) and more specifically when they involve the muscular layer of the abdomino-pelvic organs.
The endometrial-like tissue becomes fibrotic, forming nodules that can infiltrate the affected organ. Deep endometriosis primarily affects: the bladder, the ureters, the digestive tract (rectum, sigmoid colon, appendix), the uterosacral ligaments, and the posterior vaginal fornix (non-exhaustive list).
Endometriosis is classified into four stages:
This staging classification was established by the American Fertility Society (AFS) in 1979 and has been revised since 1985. It is referred to as the AFS score and is determined based on the size and location of the lesions.
It is therefore a purely descriptive classification and is mainly used as a surgical reference and an indicator of fertility prognosis. It is in no way related to the intensity of pain.
This stage can only be determined after surgery. In practice, the surgeon must count the number of lesions, assess where they are located, evaluate their size and their depth, and assign a score accordingly.
Each lesion is scored individually, and these scores are then added together to obtain a total score, which ultimately determines the stage of the disease.
01
Minimal
The stage is defined as Minimal when the score ranges from 1 to 5.
02
Mild
The stage is defined as
Mild when the score ranges from 6 to 15.
03
Moderate
The stage is defined as Moderate when the score ranges from 16 to 40.
04
Severe
The stage is defined as Severe when the score is above 40.
So...
why can endometriosis be painful?
The pain associated with endometriosis can be intense and varies greatly from one person to another. It is influenced by multiple physiological and anatomical factors.
Several mechanisms contribute to this complex symptom profile. Inflammation caused by endometriotic lesions plays a central role, as these lesions release inflammatory mediators that can irritate surrounding tissues. Muscle spasms, particularly in the pelvic floor, may also develop as a protective response to chronic pain. The location of the lesions is another key factor: lesions infiltrating sensitive structures such as ligaments, the bowel, the bladder, or near nerves can generate significant discomfort.
Hormonal activity further contributes to symptoms. Because endometriotic tissue remains hormonally responsive, it can react to cyclical hormonal fluctuations, leading to repeated inflammatory processes and pain over time.
In addition, research increasingly highlights the role of nervous system sensitization. Persistent inflammation and repeated pain signals may lead to peripheral and central sensitization meaning the nervous system becomes hypersensitive. In this state, pain can be amplified, prolonged, or triggered by stimuli that would not normally be painful.
It is important to remember that every case of endometriosis is different, and every pain experience is unique. And yet, around 10% of individuals living with endometriosis report no symptoms at all, and we still do not fully understand why.
There is still much to uncover about endometriosis, and many scientific questions remain unanswered.